Meniscal tear
KNOW YOUR MENISCUS!
Meniscus (commonly referred to as cartilage) is a wedge shaped disc of shock absorbing structure between the thigh bone and shin bone. It is important for:
- load sharing stability,
- proprioception (perception of balance),
- lubrication of the knee joint.
WHY DOES MENISCUS TEAR ANYWAY?
You may think that meniscal tear only occurs in footballers, right? You are in for a surprise…
Meniscal tear can indeed occur in patients younger than ten years. In some patients the cartilage may be formed like a slab rather than a wedge. In some patients it may not have normal attachments. In such cases minor trauma may cause tear in the cartilage. Some of these children complain of popping sensation in the knee after or during sporting activity for some time before diagnosis is made.
In teenage patients meniscus tears are related to violent sports injuries related to rugby or football. Here it is very easy to know that the knee is not right and diagnosis is made earlier.
In patients between 20-40, once again meniscal tears are related to sporting injuries. However the force required to tear cartilage tends to be less with advancing age.
In patients over age of 40 and especially over 60; a meniscus can tear easily on sudden twisting or squatting.
HOW DO I KNOW IF I MAY HAVE MENISCAL TEAR?
If you had recent tear, you may notice sudden pain, swelling of the knee. This will result in stiffness and reduced movement.
If you had tear for a while, you will notice that the knee can cause locking, jamming, snapping. It can cause swelling and reduced movements. Occasionally torn cartilage can cause a block to movement of the knee or you may notice giving way. However, after a flareup, knee can settle and may not cause any trouble for variable period of time before next flare up.
HOW DO YOU DIAGNOSE MENISCAL TEAR?
In majority of cases your history and knee examination is enough to make a diagnosis of torn cartilage.
I will check your knee to see if it has excess of fluid (effusion). I will also see if you have tenderness along the joint line where meniscus sits. I will combine it with some special tests like McMurray’s test. In this knee is bent fully, then straightened and rotated. If you have a tear in the cartilage, you may notice pain or clicking.
DO I NEED INVESTIGATIONS?
Two main investigations are x-rays and MRI(magnetic resonance imaging) scans. Not every one needs both.
Plain x-rays show bony structure of the knee. It can rule out loose bodies and arthritis. It is investigation of choice and recommended by leading knee societies in patients over 40 years.
MRI scans are increasingly performed for various conditions including knee pain. It is a type of scan that uses strong magnetic filed to produce detailed image of the inside of the body. It is a very sensitive tool and can give excellent details of the state of soft tissues in the knee.
I will combine the information gained from scan with your history and careful clinical examination to arrive at a plan.
MRI scan is not necessary when your history and examination findings are clear cut. However some insurance companies may require a scan prior to surgery to obtain authorisation.
SO WHAT DO I NEED NOW?
Don’t worry. Not all cartilage tears need treatment. If you have acute flare up or if you have recently hurt your knee; a brief period of rest, ice, elevation and anti inflammatory medicine is useful.
Occasionally minor fraying of inside margin of the outer (lateral) meniscus is identified on MRI scan. This does not need trimming.
If your demands are low and if you have recent injury, I can consider one off steroid injection.
But you have ongoing pain and mechanical symptoms for a while, you may be better off with an operation.



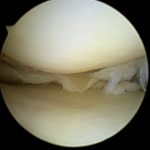
WHAT IS THE SURGERY FOR MENISCAL TEAR?
It varies. The type of keyhole knee surgery depends on:
- Your age
- Location of knee pain
- Type of tear
- Size of tear
- How long did you have tear
- Any other injuries in the same knee
- Your activity level
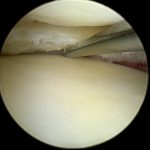
The options during knee arthroscopy are:
- Meniscal trimming (partial menisectomy, removing torn part)
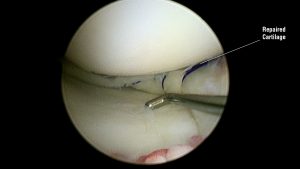
- Meniscal repair (repairing and preserving cartilage)
- Freshening of tear (for stable, small tears; roughening surface of tear will stimulate healing)
- No treatment (for certain small, partial and stable tears)
HOW DO YOU DECIDE…
Trimming of torn cartilage is the most often performed keyhole surgery. It involves removal of unstable, torn catrilage piece. Older patients especially with inside (medial) meniscal tears benefit by generous trimming of catrilage to prevent possible future recurrence.
Menisci are very important in protecting joint lining (articular) cartilage. Hence it is best to repair a torn meniscus whenever possible. The best chance for repair to work is when:
- It is a recent tear
- Tear is located in periphery of the cartilage
- Cartilage is healthy
- If you (patient) are young preferably less than 20
- If your cruciate ligament needs reconstruction at the same time
However it is a more extensive procedure than simple trimming. It has more risks and complications. Also it has up to 25% chance of failure. Rehabilitation following this is slow and prolonged and you will need brace for six weeks.
Some small tears of cartilage in otherwise stable knee can be left alone with just freshening of edge. I do this with motorised shaver like giving the edges of tear a ‘haircut’. Sometimes I make multiple punctures of meniscus with needle. Both these procedures create new raw surface and bleeding, which leads to healing. However I can only decide this during arthoscopy.