ACL reconstruction
More about ACL…
The Anterior Cruciate Ligament (ACL) is one of the main ligaments of the knee. It runs diagonally in the middle of the knee. It stops excessive movement of the shin bone in front of the thigh bone. It also provides stability when twisting and turning.
Unfortunately ACL injuries are very common in pivoting sports. It can occur during a sudden change in direction, stopping abruptly or landing incorrectly after jumping. You don’t need a tackle or physical contact to injure it either!
Of course, a tackle in contact sports eg, football, rugby, netball or handball can result in an ACL tear as well.
How do I know if I have ACL tear?
Your history, especially injury details and “giving way” of the knee will point to an ACL tear. Loss of movement, sharp pain on twisting and intermittent swelling can suggest further torn cartilage. I will check if your ACL is functioning properly by performing specific tests during your examination. I will look for abnormal movements of your knee or see if I can reproduce “giving way” of the knee.
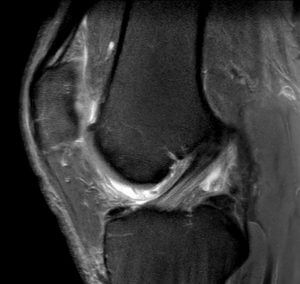
I will arrange for X-rays and a MRI scan of the knee. Your MRI scan will also show any associated injuries of the cartilage, other ligaments and bone bruising.
What do I need next?
Treatment depends on your symptoms and functional needs.
Physiotherapy
Soon after injury, most patients benefit from physiotherapy to reduce swelling, improve knee movements and to keep muscles (especially quadriceps) active. In some partial injuries, the knee may feel stable.
If the knee does not give way, you can progress well on ACL rehabilitation and may not need surgery.
Some patients can adopt lifestyle changes so that an ACL tear does not interfere with their day to day activities.
Bracing
In some cases I provide a brace due to associated injuries. Sometimes when “giving way” of the knee is very rare, patient can avoid surgery and use an ACL brace for occasional activities like skiing.
Thus surgery is not needed if:
- The knee feels stable
- Lack of compliance to therapy
- You have unrealistic expectations
- Other factors/ contraindications to surgery
ACL reconstruction: When to consider?.
One will benefit from surgery if
Knee gives way routinely
ACL tear occurs in child or adolescent
If you have associated injuries
If you have tried non operative treatment and it has failed.
Timing of operation
Have surgery when knee has regained almost full movements and swelling as well as inflammation has settled.
Get ready for surgery…
Try and get fit, cycle for half an hour every day (exercise bike)
Continue with physio and ACL rehab
If you smoke, try and quit at least for six weeks before surgery because if you smoke, you will have a much higher risk of serious complications during and after surgery.
What does ACL reconstruction involve?
Once under anaesthesia (point of no return!), I examine the knee again for final check. I then clean the knee, shave if needed and position it.
Main steps of ACL reconstruction are as follows
Graft harvest
I use single hamstring tendon and fold it four times. Unless patient has MCL sprain (ligament injury to inside of knee), I use hamstring from same knee. Rarely I sue part of quadriceps tendon above knee cap as a graft.
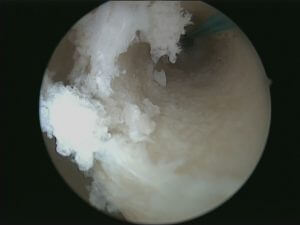
Arthroscopy
Next I perform keyhole surgery on the knee. I deal with meniscal tears by either trimming or repair. I remove any loose bodies and note state of cartilage. I try to preserve most of native ACL.
Drilling tunnels
I use special guides to position wires in footprint of native ACL. I then drill over wire to create tunnels. I also use dilator to compact bone in tunnels and thus it improves fixation of graft.
Graft passage and fixation
I pass graft through the tunnels and fix it using bioabsorbable screw in both bones. I also use back up fixation in both bones for added security. After the operation I use cryocuff to reduce pain and swelling.
COMPLICATIONS FOLLOWING ACL RECONSTRUCTION
- Infection is rare. Deep infection risk is less than 1%
- Clot in leg or lungs is also less than 1%
- Numbness around outer aspect of leg (common)
- Bleeding, swelling or stiffness (less common)
- Pain in knee may be due to associated injuries
- Failure of graft or recurrent instability (<10%)
- Damage to nerve or blood vessels (<1%)
Pain and bruising on medial side of leg and ankle can occur due to bleeding from hamstring harvest. I give blood thinning agent after operation to prevent risk of clot (DVT). Some patients can develop more bleeding due to blood thinning. However this is not serious and will settle.




PHYSIOTHERAPY
Good physiotherapy and your participation is as important as good surgery.
The goals for your are
In first two weeks;
Reduce pain, swelling, maintain knee cap mobility and MAINTAIN GOOD QUADRICEPS (thigh muscle in front). Rest your knee in between exercises. Use crutches for balance.
In the next four weeks;
Restore knee movements, improve gait, increase weight bearing and proprioception (joint position sense) so that you walk near normal. I would highly recommend exercise bike and cross-trainer.
Driving
After 2 weeks for left and 6 weeks for right knee. Return to work can be as early as four weeks for desk job.
After six weeks;
The aim is to restore normal balance, power and proprioception.
In athletic individuals physiotherapist will start advanced ACL rehab at appropriate time, usually after 4 months.
Jogging can be resumed after four months and contact sports after 12 months.